(after operation)
Article: L. BINJAKU, L. NIKOLLARI (ALBANIA)
Analysis of the Pattern of Maxillo-Facial Damage
Over a period of two years (2012 and 2013), 2129 patients with maxillo-facial trauma were registered at the Department of Oral and Maxillo-Facial Surgery in the Central University Military Hospital of Albania. The following article is an analysis of these cases, taking into consideration all data including medical history, symptoms, clinical signs, radiological findings. frequency and type of
injury as well as age and gender, cause of accidents and concomitant injuries.
INTRODUCTION
 (before treatment)
(before treatment)
Maxillo-facial injuries can pose considerable long- term functional, aesthetic and psychological complications. The management of maxillo-facial trauma includes treatment of facial bone fractures, dento-alveolar trauma and soft tissue injuries as well as associated injuries mainly of the head and neck. Trauma remains a major health and social issue throughout the world. In the United States alone, every year thousands of people of all age groups sustain facial injuries from automobile and other various vehicular accidents, firearms, athletic activities and other accidents.The impact of the driving factors on direct and indirect costs of the sequelae of trauma therapy as well as the epidemiology of facial trauma need to be allocated to their cause.
MATERIALS AND METHODS
During two years (January 2012 to December 2013), 2129 patients with maxillo-facial trauma were registered at the Department of Oral and Maxillo-Facial Surgery in the Central University Military Hospital of Albania. Data were collected including medical history, symptoms, clinical signs, and radiological findings. Frequency and type of injury (face, bone fractures, dento-aveolar trauma and soft injuries) as well as age and gender distribution, monthly and yearly distribution, nationality of patients, cause of accidents and concomitant injuries were analysed.
RESULTS
 (before treatment)
(before treatment)
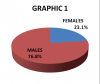
During a two-year period (2012-2013), 2129 patients were admitted to the Department of Oral and Maxillo-Facial Surgery in Albania with maxillo-facial injuries. The distribution by gender was: 1636 male (76.8%) and 493 female (23.1%) patients (Graph. 1). The prevalence of injuries was higher in male patients in all age groups. Male to female ratio was 3:1. The most frequent age group was 25 years 522 (24.5%).
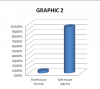
Graph. 2 shows the distribution by type of injury: soft tissue injuries: 2022 cases (94.9%) and hard tissue injuries 107 cases (5.02%).
The distribution of soft tissue injuries was: lower labii 108 (5.07%), periorbital region 773 (34.4%), facial 129 (6.05%), mandible region 348 (16.3%), nasal 232 (10.8%), upper labii 179 (8.4%), zygomatic region 85 (3.9%), laceration 106 4.9%) and intraoral 11 (0.5%) (Table 1)
Site of injuries | Nr/Percent |
Lower labii | 108/5.07% |
Periorbital region | 773/34.4% |
Facial region | 129/6.05% |
Mandible region | 348/16.3% |
Nasal region | 232/10.8% |
Upper labii | 179/8.4% |
Zygomatic region | 85/3.9% |
Laceracion | 106/4.9% |
Intraoral injuries | 11/0.5% |
Table 1- distribution of soft tissue injuries
The distribution of soft tissue injuries by age, cause and geographical site are shown in Table 2,3,4.
Age groups | Nr/Percent |
0-10 | 424/21.5% |
11-20 | 295/14.9% |
21-30 | 490/24.8% |
31-40 | 253/12.8% |
41-50 | 208/10.5% |
51-60 | 152/7.7% |
61-70 | 75/3.8% |
71+ | 74/3.7% |
Table 2 - distribution by age
Cause | Nr/Percent |
Vehicular accidents | 725/36.7% |
Falls | 624/31.6% |
Violence | 613/31.2% |
Dog’s bite | 6/0.3% |
Firearms | 1/0.05% |
Table 3 - distribution by cause
Geographic position | Nr/Percent |
Capital city | 1619/82.1% |
Rural zones | 245/12.4% |
Other cities | 107/5.4% |
Table 4 - distribution by geographical site
Hard tissue injuries were classified as: mandible fractures 83(77,5%), maxilla fractures 12(11,2%) and combined mandible/maxilla fractures 12 (11.2%), (Graph. 3).
Distribution of hard tissue injuries by cause: traffic accidents 50 (46.7%), violence 32 (29.9%), falls 10 (9.3%) and firearms 15 (14%). (Graph. 4).
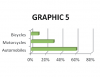
Most traffic accident involved: automobiles 30 (60%), motorcycles 15 (30%) and bicycles 5 (10%) (Graph. 5).
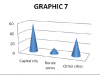
Distribution of fracture by age is shown in Graph. 6, by site in Graph. 7).
The following types of treatment of these fractures had been applied: orthopaedic 42 (40%) and surgical (osteosynthesis) 65 (60%) (Graph. 8).
DISCUSSION
Aetiology and site of maxillo-facial injuries vary depending on many factors. Most soft tissue injuries were present in the periorbital and the mandible region followed by the nasal, facial and zygomatic regions.
Many of the same principles for wound care on the body also apply to the face (wound preparation, tetanus update).


Most results of the many studies performed by different authors reveal that maxillo-facial fractures are most commonly caused by trauma such as motor vehicle accidents, assault and falls. Our own results indicate that the most frequent causes of maxillo-facial injuries were traffic accidents.
Recently, we find an increase of fractures by assault that is now the most common cause of maxillo-facial fractures in developed countries. Approximately 76.8% of the cases were male patients. This can be

explained by the fact that the majority of such causalities result from traffic accidents, violence, work-related accidents where more often men are involved. In this study, the peak incidence was in the 21-30 age group. In our study, most of the traffic accident victims were young men 18-29 years old, one of the reasons being that these men are frequently driving under the influence of alcohol or drugs. The most common site of fractures was the mandible. This observation is also in agreement with the study at ref 9. Treatment of maxillo-facial fractures varies from surgeon to surgeon. In our study, we had treated most mandible fractures by osteosynthesis and most fractures of the maxilla by orthopaedic treatment.
CONCLUSION

By analysing maxillo-facial injuries, this study revealed an accumulating risk of 92% per two years to sustain soft tissue injuries and 8% for facial bone fractures. Younger persons are more susceptible to maxillo-facial trauma. Maxillo-facial injuries occur primarily among men under 30 years of age.. Open reduction and internal fixation with miniplates is a common treatment in mandible fractures. For fractures of the maxilla, we use orthopaedic treatment. The results of our study show that road traffic accidents remain among the main causes of maxillo-facial injuries, followed by trauma resulting from interpersonal violence and assaults. This succession of etiologic factors is in accordance with the date from the most developed countries. A comprehensive education in dentistry, medicine and surgery provides these dental specialists with the skills necessary to give trauma victims excellent care.
Authors:
Lozana BINJAKU
Chief of Maxillo-Facial Surgery
University Trauma Hospital and Military Hospital
Albania Armed Forces (AAF) Tirana-Albania
Date: 07/01/2019
Source: Medical Corps International Forum (2/2015)