Article: H.B. van den Heuvel (The Netherlands)
Challenges in the Dental Fitness
Challenges for the RNDF in using Dental Fitness standards
Oral health is important for military personnel who deploy around the world. Especially for those who deploy to remote areas without dedicated dental support.
Good oral health helps to prevent Dental Emergencies.
This article aims to describe the current challenges in the Dental Fitness process in the Royal Netherlands Defence Forces (RNLDF) and to suggest possible ways of solving these issues.
Introduction
Oral health is important for military personnel who deploy around the world. Especially for those who deploy to remote areas without dedicated dental support.
Good oral health helps to prevent Dental EmergenciesI. A Dental Emergency (DE) is defined as: a condition of oral disease, trauma or loss of function, or other concern that causes a patient to seek immediate dental treatmentII.
Throughout NATO a system of Dental Fitness Standards is in use to help military dentists screen their patient population in a standardised way. Standard Nato Agreement (STANAG) 2466 describes Dental Fitness standards and a Dental Fitness Classification systemIII. There is sufficient evidence that this system, if implemented correctly, is able to reduce the number of DE’s per 1000 patients per year significantly. However, questions remain on standardisation, monitoring disease development and risk status while using the system.
The Netherlands Defence Forces have ratified the STANAG mentioned but there seem to be differences in the use of the STANAG between Navy, Army and Air Force.
This situation is not unique to the Netherlands, but seems to be present in more NATO countriesIV.
Currently the Netherlands Defence Forces and its Dental Services are subject to a major reorganisation. One of the goals of this reorganisation is a 25 percent reduction in personnel. For the Dental Services this will result in the formation of one Royal Netherlands Defence Forces Dental Service (RNLDFDS). Because of the designated reduction in personnel, the way in which military dentistry is practiced in the Netherlands needs to be reevaluated and more emphasis needs to be placed on the Dental Fitness proces in order to underline the importance of a Military Dental Service for military individuals and their respective units.
This article aims to describe the current challenges in the Dental Fitness process in the Netherlands and to suggest possible ways of solving these issues.
NL Dental Fitness approach
Although differences between the services in determining Dental Fitness exist, there seems to be agreement on the fact that Dental Fitness is determined for a period of one year. On average a Netherlands military patient will have a routine dental examinition once a year, lasting approximately 15 minutes, during which a medical questionnaire is updated and extra- and intra oral examinations are performed. If deemed necessary, radiographs are taken after clinical examination. The routine dental examination will result is classifying the patient in one of 3 Dental Fitness categories:
A fourth Dental Fitness Class exists and is used to describe military personnel who:
Callibration of military oral healthcare providers
So far only minor efforts have been made to callibrate dental personnel in determining Dental Fitness status in the Netherlands. There seems to be little or no scientific research in this particular field. Question is whether individual military healthcare providers are consistent in determining Dental Fitness classes (intra observer reliability) or whether they consistently agree with the determinations made by their colleagues (inter observer reliability). This is a serious issue, since it may result in placing patients in the wrong DF Class, which may have severe consequences during military operations.
To solve this challenge a standard set of data from patients classified in different categories needs to be assembled, in order to train military healthcare providers in determining DF status. This set needs tot be updated on a regular basis to prevent habituation to the data used. Both new military healthcare providers and those who are more experienced should be subjected to annual calibration of their DF classification skills.
Screening interval
According to STANAG 2466 the screening interval is normally 12 months, but may be set at any period between 3 and 18 months depending on the previous dental history of the individual. When treating large groups of patients that have operational obligations there seems to be a limit in awarding “individual intervals“. Currently The Netherlands digital DF module does not allow setting of intervals other than one year. This may lead to both under and over treatment for individual patients.
To solve this issue the NL DF digital module will need to undergo further changes in the future.
Capacity issues
The RNLSDFDS will have a limited capacity with which to provide oral health care. This will mean that the available capacity should be used in a smarter way. Within Dentistry there is a tendency to direct capacity towards healthy parts of the population. In the Netherlands routine dental examinations were performed on a half yearly basis. This resulted in many “unnecessary“ examinations, which gave both patients and oral health care providers an excessive sense of security but resulted in the loss of much capacity. When the Netherlands Navy changed its policies around 2003 and started using a yearly interval, it was found that this did not result in rise in DE's or a detoriation of oral health status.
Within the Netherlands Military patient population there are large groups of patients that do not require dental treatment for years. On the other hand there seems to be a group of 10–20 % of the population that is in need of frequent dental care. The DF system does not take into account these differences. To solve this issue a risk assessment tool should be added to the DF system, in order to use the limited capacity for those with the highest treatment need. However Risk Assessment seems to be a dental science in itself and international partners will have to be consulted on which type of risk assessment should be incorporatedVI.
Screening of potential recruits
In the past much dental capacity was used to screen potential recruits. Those with dental problems were sent back to their civilian oral healthcare providers. This resulted in lower recruitment numbers, because many potential recruits did not return for further recruitment after being sent away to their dentist. Furthermore the civilian dental treatment often seemed to have been performed hastily and frequently needed further correction within the Military Dental healthcare system. To achieve better recruitment figures, nearly all dental screening was stopped. This led to a higher number of recruits entering the Defence Forces with a Class 3 DF status. However average time needed to achieve DF 2 for recruits in the Netherlands was calculated to be 107 minutesVII. When reorganising The Defence Services Dentistry, this figure was incorporated into the calculation of necessary dental capacity.
Screening of recruits
Up until recently all Netherlands Armed Forces recruits underwent DF screening and necessary dental treatment during basic training. Time for screening and treatment was available in the basic training schedule. However recently we have seen a decline in available time for screening and treatment of recruits. This seems to be due to a general reduction in time available for basic training and the fact that Dental Readiness is not an end term for those in charge of this training. This recent change results in personnel arriving at their operational units or further military education, unscreened (DF4) or DF 3. In other words: the DF challenge is passed on to their new units.
To solve this issue the RNLSDFDS will ask for a change of policy which makes DF Class 2 the minimal end term for basic military training. To help achieve this, state of the art mobile dental facilities will be used to help direct extra dental capacity towards basic training facilities. Dental treatment during evenings or on weekends may also be considered.
Screening of a Dental Fit population
All military personnel are required to undergo yearly DF screening. It was calculated that the average treatment time needed to maintain at least DF Class 2 is 60 minutes per patient. This includes the 15 minute routine dental examination. In the capacity calculation for the RNLSDFDS an extra average of 25 minutes prevention time per patient was added to the total capacity in order to address an identified lack of time for preventive oral healthcare measures. There are challenges in identifying those whose DF status has expired. Although primary responsibility within the Netherlands rests with the patients and their commanders, the RNLDFDS will seek to play an active role in identifying those in need of DF classification and/or treatment. In order to play this role, DF data collection and data mining are very important.
Data input / data collection / interpretation
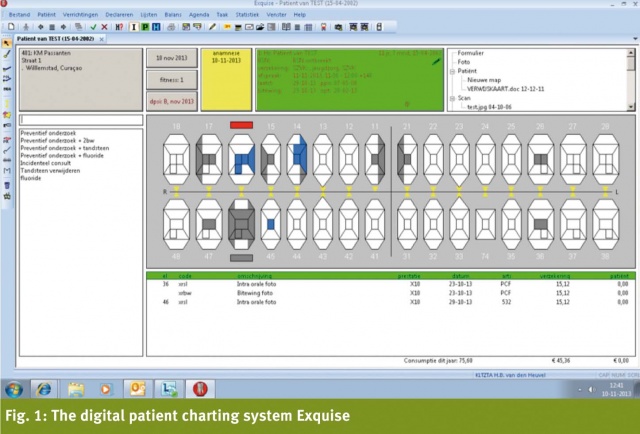
In 1998 a digital patient charting system (exquise, Vertimart Consultants B.V.) was introduced for the Netherlands Defence ForcesVIII. The system is a commercial of the shelf (COTS) system which is used in over half of the civilian dental practices in the Netherlands. The system has undergone routine adaptations for military use. Among those adaptations was the incorporation of a Dental Fitness module. A Dental Fitness category is entered by a military dentist in this module. By entering a unit identification code, a list of a units members and their DF classification could be generated. Typical unit size defined was: company, ship or squadron.

Up until 2005 these lists were routinely generated to brief commanders on the DF status of their units and to plan the use of dental capacity for those with the highest needs.
In 2005 a new digital personnel system (peoplesoft) was introduced for the Netherlands Defence Forces. This system used a radically different approach to identify units. The introduction of this system effectively blinded Exquise and made the DF module unusable.
In subsequent years no funds were available for adaptation of the DF module to the new system and the idea of a corporate data system that would be able to generate all data needed by commanders became leading. During this period the directors of Dental Services made a constant effort to get the DF module restored, arguing that they were supplying the DF data, but were not able to benefit from it and use it for capacity planning.
Exquise does report DF data to the peoplesoft module. Line managers are able to see the DF status of their personnel, but the system only differentiates between Yes (DF 1/2) or No (DF 3/4) and gives the DF expiry date.
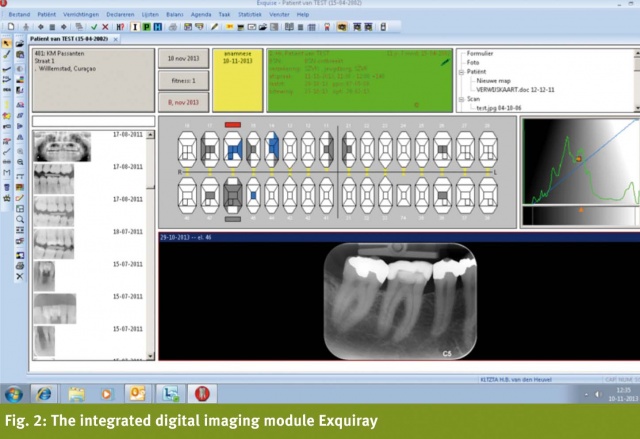
After eight years of stressing the importance of DF status for Military Dentistry, a new version of Exquise, being introduced in November 2013, will finally restore the function of the DF module. This new version will also communicate with the EMPIC system in which data for aircrews and their flight medical condition is stored. The flight surgeons using EMPIC will be able to see the current DF status in their system and dentists will be able to see whether a person is under flight medical screening and therefore needs to be DF Class 1.
The introduction of the new module solves a lot of issues in data entry and data mining for the RNLDFDS, although after eight years it may take some time to get accustomed to using the system to its full potential.
Furthermore, a proposal for identification of other groups with special DF needs (e.g. special forces, divers, and submariners) is being prepared by the RNLDFDS.
Data infrastructure
In order to use Exquise and the DF module to its full extent. Every operato needs to have direct access to the Eexquise server. Since military dental operatories can be situated in mobile clinics, on board of a ship and in the field, real-time access may be considered a serious issue.
Up until now while practicing dentistry during deployment dentists would use a standalone version of Exquise or use small bandwidth lines of communication with the server. Both methods have serious drawbacks. To solve this issue the requirements for the future data infrastructure of the RNLDFDS was formulated as follows: “24/7, secure, real-time, broadband access to the Exquise database anywhere in the world.“
Recording and sharing DF information among NATO partner countries
Nowadays most operations in which the Netherlands Defence Forces are involved are combined operations with NATO partner countries. Military Dental Teams deployed during these operations will see patients from many different countries. Different countries use different forms for Dental (Emergency) data collection and the DF Class of a foreign military patient is usually unknown. In order to collect better data during operations, agreement should be reached within NATO on a standardised dental data collection form to be used during combined operations. Furthermore, DF classification data of all international units taking part in combined operations should be made available to the countries supplying Dental Teams in order to plan in accordance with this data.
Although there is longstanding agreement on how DE data should be collected, to the knowledge of the author there is no NATO standard form to record this dataIX. If possible the STANAG 2466 should be expanded with such a standard form. Using such a form during all types of practice will probably produce more reliable data on DF classification in the future.
Two steps in classifying DF 3
If a patient is classified as DF 3, he is an immediate burden on the deployability of his unit. Within the military system classifying an individual as DF 3 should therefore immediately be followed by an assesment of the individual deployment needs of that patient and those of his unit. If the patients unit is not going on exercise or not deploying within the next few months, normal treatment planning is initiated. However if the patients unit is going on exercise or deploying in the near future, a fast track dental treatment planning proces should be initiated. This fast track proces should incorporate all preventive and curative measures needed and allow for sufficient time to evaluate the treatment performed, before deployment. In some case this may mean that an individual patient will deploy later than his unit. Utmost care should be taken to prioritise dental capacity towards deploying personnel classified as DF 3. In the Netherlands it has been found that some military dentists seem to consider this system unjust, because “dirty mouths“ are given priority over “clean mouths“. In the future the RNLDFDS will address this issue more carefully and consistently, so that individual dentists will be better suited to support the military system of prioritising care to DF 3 patients.
DF standards versus Evidence Based Guidelines
In 2012 The Netherlands Health Council published a report titled “the oral healthcare of tomorrowX“. In this report it is concluded that there is a serious gap between science and treatment within dentistry, both in the Netherlands and the rest of the world. The Netherlands dental community is urged to formulate treatment goals, develop evidence based treatment guidelines, to collect treatment data in a standardised way and to form a network of practices affiliated with the academic dental centres in the Netherlands.
It is a goal of the RNLDFDS to follow these recommendations.
The DF system seems to be a good basis from which to achieve this goal, although additions to and adaptation of the system seem necessary. Treatment goals could be defined on an individual patient basis: minimal DF Class 2 or on a unit basis: 90% DF 2 minimum.
The fact that one digital system is in use should help in entering and collecting the treatment and outcome data in a standardised way.
Although a good scientific basis for the use of DF standards seems to exist, the individual parameters such as “there is no evidence of active periodontal disease that is beyond control by self-care“ seem to lack a sufficient scientific basis.
To solve this issue we suggest that a future Dental Fitness guideline should be developed according to the AGREE II instrumentXI.
The Defence Forces Dental Services have a long standing affiliation with departments in the Netherlands Academic Dental Centres. In the near future we hope to start cooperative projects in which academic researchers may use our digital dental treatment data, accumulated over the past 15 years. For prospective public health studies, the RNLDFDS seems to provide an ideal research model. A large practice with 42 000 patients, one treatment protocol, one digital database and 14 clinics distributed across the Netherlands.
Furthermore the RNLDFDS is closely following the development of a new organisation, that will develop national evidence based clinical treatment guidelines. This initiative was given the preliminary name “Chamber for Oral Health Care“ and at least one member of the RNLDFDS is taking part in this initiative.
What if NATO DF standards seem contrary to national oral healthcare guidelines?
Netherlands’ dental professionals have to adhere to Netherlands standards of care. As stated above there is a lack of good dental guidelines in the Netherlands, but a guideline that may conflict with DF standards has been identified.
The Netherlands’ guideline on removal of impacted lower third molarsXII.
Whereas The STANAG states that individual occupational and operational commitments must be taken into consideration, the Netherlands’ guideline only considers the clinical and radiographic aspect.
Following the Netherlands’ guideline may lead to more erupting molars causing problems for individuals and units, whereas following the STANAG may lead to over treatment and unnecessary preventive removal of molars.
To solve this issue more data on problems during deployment specifically originating from third molar pathology should be collected in the future.
As mentioned above, a new initiative to develop evidence based clinical treatment guidelines has been taken in the Netherlands. The RNLDFDS will closely monitor whether newly developed guidelines seem to conflict with the DF classification system, and will work closely with all parties concerned in order to keep the DF classification guidelines in accordance with the Netherlands standard of care.
Special DF demands for specific groups of military personnel
In the Netherlands Defence Forces special groups of patients have special Dental Fitness Class demands. As mentioned above active flight personnel require DF 1, as do Divers, and submariners. It is unclear why these special demands exist.
There seem to be historical reasons based on the supposed prevention of barodontalgiaXIII in DF 1 patients. To the knowledge of the author there is no evidence base for the special treatment of these groups and there are no studies linking DF class to the prevalence of barodontalgia. Although not supported by evidence the special demands have resulted in the fact that the groups mentioned may claim 100% reimbursement for fixed prostodontics, where as other groups are only partially reimbursed in the Netherlands’ system.
The author recognises the fact that certain groups of military personnel require perfect oral health because of the work they do, but future research should be directed towards the ability of the current system to prevent barodontalgia.
In this light it seems strange that so far special forces, whose modus operandi often exposes them to remote areas, without access to oral health care, are not required to be classified DF 1. The RNLDFDS should look into the policy regarding special groups of patients and formulate a new set of demands based on specific occupational demands such as flying, diving, playing a wind instrument, or working with mission profiles that do not allow dental treatment for extended periods of time.
Conclusion
The system defining Dental Fitness classification standards forms the backbone of military dentistry. However many questions and challenges surrounding this system remain.
The Defence Forces Dental Services in the Netherlands are undergoing major reorganisation. The future Royal Netherlands Defence Forces Dental Service (RNLDFDS) aims to play a significant role in addressing these challenges and helping to answer the remaining questions. n
References: ref@mci-forum.com
The opinions expressed in this article are the private views of the author and should not be construed as reflecting official policies of the Netherlands Defence Forces, the Netherlands Department of Defence, or the Netherlands Government.
Date: 01/26/2014
Source: MCIF 1/14