Article: Brig Harjinder S Bhatoe VSM
RETAINED INTRACRANIAL SPLINTERS: A REVIEW
With rapid evacuation of patients with craniocerebral missile injury (CMI) from the combat zone to neurosurgical centers, early evaluation with computed tomography (CT), improved surgical techniques and post-operative care, there has been an overall improvement in the survival of these patients. Series have reported improved survival even in patients with low Glasgow Coma Score (GCS) (Levy 2000). This has also resulted in more survivors with retained intracranial splinters, who have been followed up over a period of years, and their sequelae and outcome have been studied. The veterans with such a problem may attribute a number of symptoms and problems with retained intracranial splinters. Since the number of personnel with retained intracranial splinters might be rising, there is a need for renewed awareness of the implications of retained intracranial splinters amongst the patients, their family members, the primary care physicians, etc.
REVIEW OF THE PROBLEM
 CT showing intra-third ventricular
splinter
CT showing intra-third ventricular
splinter
Splinters either with insufficient residual kinetic energy (KE) to exit the skull or exploding bullets that rapidly release their KE get lodged intracranially. Retained intracranial fragments may be survivors who have not been operated upon, or those who have retained fragments despite debridement. These fragments are generally low velocity missiles such as pieces of shrapnel, shotgun pellets, secondary missiles or bone fragments. Retained intracranial splinters posed a dilemma for several years till their sequelae were understood during the course of follow-up studies of survivors of various wars.
In Cushing’s experience in World War I, intracranial infection was the major cause of mortality (Cushing 1918). Although he advocated removal of devitalized nervous tissue, Cushing also believed that deeply embedded foreign bodies should not be removed at the risk of aggravating the neurological damage. However, subsequent military neurosurgeons believed it was imperative to remove all intracranial bone and metal pieces in a patient with splinter injury of the brain. Reoperation was advocated if retained fragments were evident after initial debridement (Hammon 1971, Mathews 1972). One of the primary concerns of such an aggressive approach was the fear of infection and formation of inracerebral abscess (Meirowsky 1968). Based on their World War II experience, Martin & Campbell (1946) recorded a parenchymatous infection rate of 16%; they believed that infection was ten times more likely to occur in the presence of retained bone fragments than in their absence.
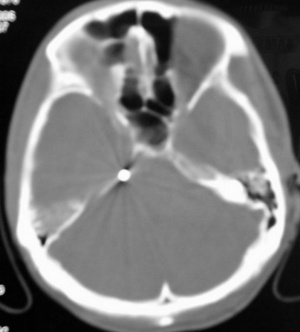 CT showing splinter
over the right petrous surface
CT showing splinter
over the right petrous surface
There has been a change in approach, beginning probably from the experience of Brandvold et al (1990) in Israeli soldiers injured during the Lebanese conflict. With the availability of CT for immediate evaluation of these patients, a less aggressive approach was formulated and adhered to, with emphasis on preservation of cerebral tissue, and removal only of in-driven fragments that presented themselves on gentle irrigation during haemostatic manoevres. With this less aggressive approach, 60% had retained metal or bone fragments (or both). The acute outcome with respect to complications and mortality was similar to that reported in Vietnam series. No relationship existed between the presence of either a seizure disorder or subsequent CNS infection (Table 1). Based on their experience with 379 patients during the Iran-Iraq War, Aarabi (1987) concluded that site of injury and retained splinters did not have correlation with CNS infection.
SEQUELAE OF RETAINED INTRACRANIAL SPLINTERS
Majority of the retained fragments lie dormant, and cause no further problems, although the patients might attribute a number of non-specific symptoms to these fragments. We have seen small fragments lie embedded in the lateral ventricular wall, or in the third ventricle. One patient with a small retained fragment lying along the petrous ridge on the right side presented with trigeminal neuralgia, which responded to carbamazepine. Retained intracranial splinters have been implicated in the genesis of the following sequelae:
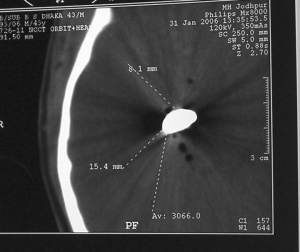
 CT showing retained metallic splinter
after orbitocranial injury
CT showing retained metallic splinter
after orbitocranial injury
Infective complications: Splinters that have transgressed the face, sinuses, orbit and skull base, and those that are accompanied by CSF leak, brain matter herniation and brain swelling are the ones that may be followed by repeated episodes of pyogenic meningitis, ventriculitis, requiring frequent, full course of appropriate antibiotics. Episodes of meningitis may commence within two to three weeks, or may occur after months. These episodes may be followed by obstructive or communicating hydrocephalus. Brain abscess may form after these episodes of meningitis in the later months or years, or they may form during the first few weeks of the injury. Intraventricular lodgement of the missile predisposes to infective complications (Clark et al 1986). Entry of the missile through the skull vault is less often associated with infective complications (Aarabi 1987, Bhatoe 2001).
Illustrative case: A 45-year-old soldier sustained right orbitocranial splinter injury in 1989, while serving with the Indian Peace keeping Force. There was no focal motor deficit. His right eye had to be enucleated, and limited debridement of right frontal region was carried out. Metallic splinter could not be removed. CT brain showed retained metallic intracranial fragment. Over the next four years, he suffered from five bouts of pyogenic meningitis, each time treated with antibiotics. In 1993, he was admitted with headache and two-week history of hemiparesis. CT brain showed thick walled brain abscess with vasogenic cerebral oedema, and metallic splinter adjacent to the abscess. The abscess was excised together with the splinter. Pus was sterile for aerobes and anaerobes. He showed recovery from hemiparesis over the next six weeks. However, six months later, he was readmitted with headache, and this time CT showed hydrocephalus. He underwent ventriculoperitoneal shunting and remained asymptomatic thereafter.
Epilepsy: There is no definite correlation between occurrence of epilepsy and retained itnracranial splinters (Aarabi et al 2000, Brandvold et al 1990). The pathogenesis of epilepsy after CMI probably involves the formation of an epileptogenic focus, and about one third to one half of the survivors with CMI can be expected to develop epilepsy.
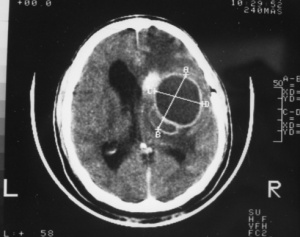 CT showing formation of brain
abscess with splinter embedded in the
abscess wall
CT showing formation of brain
abscess with splinter embedded in the
abscess wall
Migration: Besides infection, intracranial migration is of serious concern. A migrating missile can result in worsening of neurological deficit due to passage of the bullet through the eloquent brain. These fragments may be intraventricular, intraparenchymal or subarachnoid in position. When intraventricular in location, these fragments may shift their position because of availability of space around them, and have been implicated in the pathogenesis of hydrocephalus, ventriculitis, hypothalamic dysfunction, etc. (Dagi & George 1995). Migration is less often seen in intraparenchymal fragments, since they are surrounded by tissue or gliosis. Migration can occur soon after the injury along the corridors of tissue damage created by tumbling or yawing passage of bullet through the brain. Movements are aided by bullet weight (heavier bullets tend to shift their position), gravity and brain pulsations and “sink effect” of the ventricles of the brain (Rengachary et al 1992, Milhorat et al 1993). Delayed migration indicates softening of the surrounding brain, while arrest of migration can occur due to oedema, gliosis and due to the fragment getting embedded in a developing brain abscess. Subarachnoid migration can occur through CSF pathways. Infarction can result from vascular occlusion (Chapman & McClain 1984). Cerebral aqueduct can get occluded by wandering fragments causing hydrocephalus (Lang 1969, Ott et al 1976). Fatal migration into the brainstem has been reported (Ott et al 1976).
MANAGEMENT STRATEGY
A retained intracranial splinter is a cause for anxiety and concern to the patients and the relatives. What is needed is a clear understanding of the nature of the cerebral injury, and communication with the patients and their relatives explaining the need for regular follow-up, and close observation for neurological deterioration. While meningitis will be diagnosed and treated in the usual manner, any fresh neurological event mandates evaluation by imaging. Brain abscess may require to be excised and often the missile is found adhered to the abscess wall. There is no aggravation of deficit due to excision of the abscess. Migrating missile may require appropriate image guided management strategy. Removal can be affected by CT guidance or in case of fragments lying on the cortex, by taking skull radiographs or intraoperative CT in the operation theatre to localize them precisely immediately prior to or during craniotomy. Care should be taken to minimize dissection or retraction of brain tissue so as to avoid worsening of neurological deficit.
Author
Brig Harjinder S Bhatoe VSM
Director and Chief of Neurosciences
Max Super Speciality Hospital
Patparganj, IP Extension
New Delhi 110092. India
Address for correspondence:
Brig Harjinder S Bhatoe VSM
Director & Chief Neurosciences
Max Super Speciality Hospital
Patparganj, IP Extension
New Delhi 110092. India
Tel: 91-120-4274980
Date: 01/10/2019
Source: Medical Corps International Forum (1/2014)