Report: F. HENGSTERMANN (GERMANY)
Medical Support of Infantry Operations
Experiences of a medical officer serving with the Task Force Kunduz in 2011
The author reports on his personal experience during an 8 ½ months’ deployment to Afghanistan. In the way of a “lessons learned”, he refers to diverse viewpoints he encountered and accounts of various impressions – not limited to his field of profession as a medical officer. He concludes with his personal survival strategy - good advise to anyone transferred to a similar situation.
Introduction
As a serviceman and medical officer with relatively extensive experience of service in the field as well as medical proficiency, I was posted for a longer period of deployment with ISAF in Afghanistan, where I encountered diverse viewpoints, impressions and new experiences. Being deployed in the field for a period of 8½ months was also presented a constant and not at all trivial challenge. I was able to contribute in terms of both medical and leadership skills; moreover, it proved both instructive and useful to gain insights that went beyond those of my medical activities alone. Although I cannot go into extensive detail with regard to everything I experienced within this article, I hope that the following will prove to be of value to many readers.
The German military medical services have in recent years risen to the challenge; they are doing a good job in many areas – even within the poorly defined situation on the frontline – so that their reputation within the German Armed Forces as well as with other military forces and around the world at the moment seems to be particularly high. We can be justifiably proud of our achievements and the proficiency of our personnel.
Background to deployment – how did it happen?
The demands being faced by the German Armed Forces (GAF) in general and in the various individual areas have undergone a fundamental transformation since the end of the Cold War. The principles and techniques, structures and focus of the GAF are subject to continuous and sustained evolution. It has become a major problem to keep oneself fit with regard to comprehension, expertise and even skills in order to be up-to-date and combat ready. This applies particularly to personnel of all ranks who had been serving with the forces in the old days of the Cold War and who had received their training and thus formed their essential outlook during this period. This is something that I myself could recently witness and also experience in my own case.
At the beginning of my medical career and in addition to acquiring a qualification as a specialist in ENT medicine at GAF Hospital ULM, I also received training in emergency medicine with a view to my deployment in the field. Directly following completion of the first clinical phase of my course, I required this training to serve with the UMOMIG in the Caucasus in Georgia. Here, at a relatively young age, I gained a wealth of experience, insight and understanding of the military, medical and human factors involved. I also discovered the benefits of broadening my horizons – it was by no means standard practice at the time for a specialist in one of the more 'minor' disciplines (ENT) to train in emergency medicine. My deployment lasted 6½ months, a period of unarmed service during which I was exposed and vulnerable, but was also able to explore my options for independent medical and military participation. In common with most extensively trained UN observers, in 2004 I again had the opportunity after 1999/2000 to employ what I had learned.
After obtaining my qualification as a specialist, the logical consequence was my further employment as an ENT physician; as a member of KFOR in 2004/2005, I got to experience a completely different situation and alternatives in the Prizren field hospital. In a context where you are not required to work alone but as part of a clinical team with all its expertise, its members representing all medical disciplines and its access to apparently inexhaustible resources, you almost feel that the facilities are those of your own GAF hospital back in Germany and that you are thus in a situation where an optimum level of care can be provided. You are able to employ your acquired and standardised skills in an environment with which you are familiar; the only difference being that you are far away from home. Deployment there was characterised by the thoroughness resulting from the use of accustomed procedures.
But the situation was to change drastically and the medical services also had to modify their profile accordingly. In contrast with the conditions in UNIMIG in Georgia, the spotlight was turned on emergency medicine – the medical services recognised their responsibilities as a service provider and managed to put together a larger contingent of experts in emergency treatment. Considerable numbers of paramedics and subsequently field medics were also trained as a consequence. With the exception of those in a few disciplines (those without direct therapeutic relevance to patients), all trainee physicians/ medical officers were encouraged to study emergency medicine during the first clinical phase of their courses. There may have originally been resistance because of an unwillingness to accept and comply with this, but this was very soon replaced by the realisation that this was what was required. I witnessed all this while working as a personnel manager in the personnel department and later as a personnel consultant in the German Ministry of Defence (BMVg). The requirement may have been recognised and appropriate measures introduced, but the approach was far too abstract.
Deployment as a planned strategy
Although I had been serving as commander of a Kempten-based mountain medical regiment (GebSanRgt 42 'Allgäu') since July 2010, it was decided to transfer me to ISAF from November 2010 because the task force had an extensive need for medical officers/physicians, particularly those versed in emergency medicine. My assignment was to take over command of a contingent of our medical evacuation company (MedEvacKp) in Mazar-e-Sharif. I was aware that not only would I have the task of commanding the contingent but that I would also be employed as an emergency physician with a mobile medical team (BAT) as I had worked in emergency medicine for the previous 14 years in Germany and had also been able to use my skills in this area, as described, during my deployment with UNOMIG. At last November 2010 came and, after a relatively brief period of field training, I was sent to Afghanistan. The reality of serving in the field catches up with you sooner than you might think: after just 24 hours of transfer discussions and instruction, I was given official command of the company. The MedEvacKp represents, as it were, a hotchpotch of the various medical emergency services deployed in Mazar-e-Sharif. There are ground-based emergency teams and BAT teams issued with YAK-class vehicles. There are also the components required by structural planning, such as the troop physician and dental/oral physician groups based in the field hospital; these have been assigned to the MedEvacKp because of their participation in role 1 medical support (Fig. 1). Also part of the company are the air evacuation units using CH-53 helicopters and Transall C 160 transport aircraft.

This was an interesting assignment for me, as I was working both as a level 1 commander with responsibility for discipline and as a doctor and emergency physician within the military network. Not only this, but I was also appointed Medical Incident Officer (MIO) of Camp Marmal in Mazar-e-Sharif and Anaesthetics Officer (BTM) for the whole camp and all units based there. Because of the many medical teams with their major reserves of opiates and morphine autoinjectors to cover the needs of all personnel serving with the units in Mazar-e-Sharif, this is a job that is not exactly a pushover and is unfortunately associated with considerable administrative paperwork. In view of the legal regulations that apply to the management of opiates, extensive monitoring is necessary; any discrepancies with regard to stocks (i.e. disappearance) of opiates could lead to major problems.
In the civilian context, the post that I was assigned to, with its various facets and responsibilities, would probably be called 'Head of Emergency Medicine'.

The various resources available to the company are used as need dictates. The airborne units are thus used to transfer casualties, particularly those with serious wounds, from the strategic front line with provision of a high standard of intensive care to the field hospital in Mazar-e-Sharif (Fig. 2). In Kunduz, for example, it was often the case that casualties were first stabilised in a role 2 emergency centre and then flown to the field hospital where they could be provided with optimum medical care (role 3). I could fill in a lot of details here, but I will simply say that the field hospital is provided with all the diagnostic and therapeutic resources and specialist personnel essential to the task. The standard is similar to that to be found in a university hospital.

The armoured ground-based ambulance vehicles, such as those of the YAK-class (see Fig. 3), accompany military police units and other groups on their daily rounds and patrols, or supplement the medical resources available at satellite camps, such as Camp Spann, where the Afghan security forces (army [ANA] and police [ANP]) are being trained.
There is no doubt that the predominant factor in the case of Mazar-e-Sharif is that it is the location of the headquarters of German-led ISAF Regional Command (North) – the C in C was originally Major General Fritz, who was succeeded by Major General Kneip. Additionally of importance is the fact that Mazar-e-Sharif is, as the main camp of RC North, the logistical hub and access point for all supplies; most active operational units and their staffs are based here. There are also units of the forces of other nations, such as the USA, Sweden and Norway together with a large airfield, meaning that some 10,000 personnel are now stationed there – with quite extensive ramifications.
Because of the centralised command function of the camp and the fact that the threat level here was low, I found living and working here to be both safe and unintimidating. On leaving the camp, however, one can encounter situations so very different that one is left in a split mind. You leave the camp with its many facilities and relative security to go on missions involving considerable risk and uncertainties, only to return subsequently to the shelter of the camp. The majority of personnel remain there the whole time (they are on staff duties). You can often feel that the camp is an unreal world on your return, particularly when you witness the problems, distress and worries that some of your fellow service personnel experience. You discover the concepts of 'insider' and 'outsider': groups tend to form on the basis of the actual or perceived responsibility, risk and strain that each is subject to.
New situation, new challenges and decision to accept the situation
I had hardly settled in before Operational Command in Germany contacted me with a problem. The designated commander of the mobile medical company in Kunduz (see below) who was to take over in January 2011 was unable to take up his duties. Despite an extensive search it had proven impossible to find a suitable replacement – it was felt inappropriate to assign a young medical officer with little field experience to the post while it would require at least 5 - 6 months of training to prepare someone for this task. The mobile medical company in question (SanKp bwgl Eins KDZ), provides medical support to the training and security battalion in Kunduz (i.e. the Task Force Kunduz) and thus represents the most robust and demanding infantry-attached unit maintained by the GAF medical services and enjoying top priority. Considering my military experience, it was felt that I could assume this post without the extensive and related training that would otherwise be required. Although this meant a significant prolongation of my period of deployment and would considerably delay my return to my regiment in Kempten, I recognised that this was my duty and decided to accept the challenge. What was originally to have been a 4-month tour of duty in Mazar-e-Sharif turned into 8½ months, 6 of which I spent with the Task Force Kunduz.
New base of operations in Kunduz
In January 2011, I found myself in command in Kunduz just as rapidly as I had been inducted into the company in Mazar-e-Sharif. Kunduz is the 'hot spot' for the German contingent of ISAF. The Task Force Kunduz, originally formed from the Quick Reaction Force (QRF), is the German unit that is most exposed and most in action. It has to live with a situation where threat is commonplace. I gradually took charge of the personnel deployed to my company who were on a six-month tour of duty. I laid down the strategy and requirements for myself and particularly for the young men and women of my company. I needed to establish contact with the other unit commanders, the Task Force command, as rapidly as possible as we would be working, fighting and thus surviving together over the long term.
On the Task Force itself:
Officially only a 'guest' in Kunduz field camp, a place that lacks all the amenities and 'luxury' facilities to be found in Mazar-e-Sharif, the mission of the Task Force was to maintain security in its assigned Area of Responsibility or 'OpsBox'. The Task Force Kunduz was of battalion size, consisting for the main part of an infantry battalion (in our case, the Parachute Battalion 263 from Zweibrücken), with a battalion command staff and various infantry companies, supplemented by so-called 'enablers'. These were two mechanised infantry units (integrated in the paratroop companies), an engineer company, a reconnaissance company and a medical company, the latter dependent on cooperation with the other units as it was officially part of the medical field group. The term 'enabler' is particularly appropriate with regard to operations – the combat troops are only able to undertake missions successfully with the support of these specialised military units and these are so essential that such missions would be otherwise impossible.
Thus, together with the first level units and their numerous important functions such as maintenance, recovery and transport (Fig. 4), there were basic G 2 support elements (military communications) and civil-military co-operation (CIMIC) units, the two infantry companies with the stated reconnaissance, engineer and medical companies – in total six companies formed the field force.

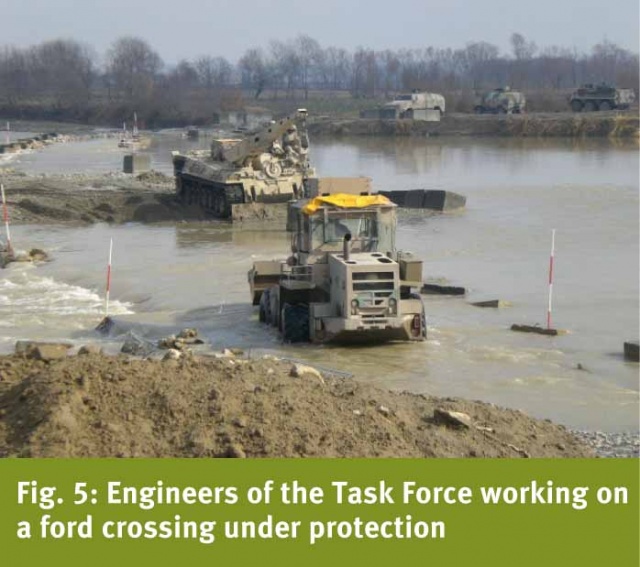
Essential for the mission was the ability of all units to act in concert with the infantry while performing tasks under combat conditions. In addition, these activities were supplemented by other special skills, such as mine clearance, reconnaissance and medical support. Missions were almost always undertaken by the various units acting as a group. This strategy was previously known as use of 'combined arms' – a term which has now taken on a very real meaning for me. In situations in which the engineers are required to construct secure positions (checkpoints or combat outposts) or improve a ford (Fig. 5) under fire and, under similar conditions, the medics need to tend to casualties and evacuate these by land or air, it rapidly becomes clear that everyone needs to pull together.
Irrespective of whether the mission involved securing territory (i.e. holding already controlled areas), patrols in controlled zones or those in which insurgents (the Taliban) were present, or operations to gain territory – the only option was to work together.
These experiences, including that of working in an atmosphere of genuine mutual support, were of considerable value for me personally. It was also very satisfying to observe that the prestige enjoyed by many of the enabler units was significantly enhanced because of this co-operative approach and also because of their willingness to carry out their duties under given conditions. It is for this reason that the mutual respect between the various branches of the services and particularly the perception of specialised skills, such as logistics, maintenance, engineering and medical support, is now better than ever. I feel competent to say this with some justification, having served in the GAF for nearly 23 years.
But there is a downside to everything...
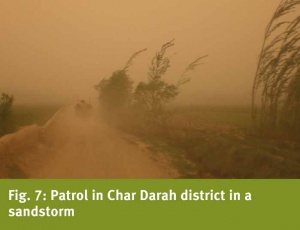
Despite all the positive and interesting experiences, it is impossible to forget the strain of having to live and work in extreme conditions while placing one's own life on the line. The recurring long periods of duty in the combat zones far from any field camp, the very sparse living conditions, the awareness of being constantly exposed to threat, the exhausting physical work outdoors, the repeated experience of being under fire, the psychological stress, the loss of comrades of all nations – all this takes its toll and can prove to be too much for some individuals. Patrols under apparently controlled conditions (Fig. 6) can suddenly be transformed into a challenging situation (Fig. 7).

I can clearly remember my first experience of duty under fire when, as an Initial Reaction Force, we were instructed to relieve a unit that had been ambushed. The feeling on the way to the TICs (troops in contact) was difficult to describe, but predominant was everyone’s hope that we would be able to extract our comrades.
I can recall many MedEvac operations in which, thanks to excellent overall work, the skilled and courageous efforts of medical service personnel and a, by then, perfectly functioning rescue chain, it was not only possible to recover wounded personnel but to restore them to health through corresponding treatment and follow-up care. But I also remember many instances of attacks with improved explosive devices (IEDs) and memorial services for fallen comrades (Fig. 8). And I can recollect the associated feeling of powerlessness and helplessness, followed by the difficult task of pulling oneself together and neither losing hope nor overreacting. In my role as commander, I had to provide a particularly good example in such situations and provide clear leadership and character guidance. Whether those who have undergone such experiences place much value on receiving an award or combat medal may differ from individual to individual. For myself, I can only state that I am primarily glad that I not only survived, but was also able to return completely unharmed. And I am pleased that I have been able to take up my normal life again in my homeland, in Germany. Not everyone is as lucky as I have been. During the debriefing seminar on our return from the mission, at least one in every three of the personnel in my company was still suffering from the after-effects of their experiences. Some will probably never manage to overcome the associated problems. So I am all the more pleased for those who are able once again to enjoy life to the full.
Other thoughts and long-term considerations
There are certain things that impress you while on active service and that remain in your mind and to which you keep returning. One such aspect is the nature of the mission and the participation of the medical services. It is understandable that as a non-combatant, you may have concerns about being involved in such precarious situations. The rights of the medical services in this respect do need to be taken into account. But at the same time, the combat troops being supported cannot be left alone but must continue to be provided with the professional care to which they are entitled. This does mean, however, that our personnel as non-combatants must also be trained to survive during missions in such a harsh and dangerous environment. The basic equipment required for self-defence must also be provided (Fig. 9).

As medical personnel, we don’t need to fear comparison within the larger organisation of the GAF. Thanks to the systematic adaptation of equipment, training, organisation and procedures, we now have a system of field medical support that is excellent. But we cannot simply rest on our laurels; we must actively seek out potential for improvement. At the same time, we can justifiably look at what we have achieved and conclude that what we are doing is unbelievably effective. From the front line to definitive, central clinical treatment, we provide a level of care and outcome for wounded and sick personnel which other systems can only dream of. The infantry personnel are well aware that their comrades are very rapidly transferred to a facility in Germany where they can receive the best level of treatment, that they will survive and perhaps even be returned to duty, and that this is only made possible by all the many links in the rescue chain. We can be proud of this and can self-confidently broadcast our successes.
But what is the best way to get through such a long and demanding mission without suffering permanent trauma? For the situation I was in, I managed to develop a very simple strategy that would ensure that I would return home sound in body and spirit. This involved:
- Acceptance of the given situation
You need to simply go along with the fact that you are on deployment and accept the situation in the same way as the assignment. Questioning and indecision will not help matters. It will only make you uncertain and will restrict your ability to act if you worry about why you are where you are.
- Target your day of return
Irrespective of the duration of your tour of duty, make sure you are ready and fit to be returned and reintegrated in your environment at home.
- Try and retain the basic elements of your normal style, decorum, habits and outlooks
Although it is not possible to completely avoid the use of language suitable to the situation, you should never allow yourself to excessively indulge in this. It may be considered okay to use certain words and phrases repeatedly in the field, but back home their use will only confuse and could even disconcert your listeners. Retain your normal speaking style.
- Maintain extensive contact with home and show interest in what they have to say
Irrespective of how mundane and unimportant information and news from home may seem to you – this is the world that awaits you when your tour of duty is over, and where you will need to reintegrate yourself. Stay in touch as much as possible because that means it will be all the easier to become part of it all again. And hearing about the happenings and problems at home makes you aware that there is more than your tour of duty that is important to you.
The described impressions, events and experiences and the long duration of deployment – these are things that unavoidably leave their mark on you. At the same time, I am glad that I have been able to supplement my own perspectives and that I have been able to return home unscathed. I am also pleased about the additional confidence and the evidence I have seen of the valuable role being played by the medical services in the German Armed Forces, its work and achievements.
Author
Lt Col Dr Frank Hengstermann
Dept. of Tropical Medicine of the Bernhard Nocht Institute
Born: 8 April 1970 in Rosenheim, Upper Bavaria
1989 – 1990 Joined the German Armed Foces (Bundeswehr) in Rennerod (Westerwald) as a medical officer cadet;
Basic training and subsequent training (trainee ensign,
officer cadet); 1990 – 1996 Study of medicine; 1996 Licence to practice; 1997 Doctorate; 1996 – 1999 Specialist medical training/First clinical phase ENT at GAF Hospital Ulm; 1999 Qualification in rescue medicine, subsequently emergency medicine, emergency medicine consultant, director of rescue medicine; 1999 – 2001 Service as a medical officer airborne corps/airborne medical team Altenstadt, head of on-call medical services and airfield aviation medicine; 2001 – 2004 Continued specialist training/Second clinical phase; 2003 Flight Surgeon; 2004 ENT consultant; 2004 – 2008 Head of Clinical Disciplines, Personnel Department; 2008 – 2010 Consultant to Ministry of Defence (Personnel Manager and Consultant) in Bonn; Since 2010 Commander Mountain Medical Regiment 42 'Allgäu' in Kempten; Foreign tours of duty: UNOMIG Georgia (JMO) Oct. 99 – April 01, UNOMIG Georgia (JMO/SMO) March 04 – June 04, KFOR Kosovo (as ENT physician, field hospital) Dec. 04 – Jan. 05, ISAF MeS (Company Commander MedEvacKp) and Kunduz (Company Commander SanKp bwgl Eins KDZ) Nov. 10 – Aug. 11
Date: 08/12/2014
Source: MCIF 3-14